First10EM Journal Club: August 2021
Welcome backk tot he Journal Club with Justin Morgenstern and I prattling on about all sorts of ED EBM goodies. 80 miinutes, 10 papers and many opinions… enjoy.
Antibiotics won’t work for your virus, but take these antibiotics in a couple days anyway
Mas-Dalmau G, Villanueva López C, et al. Delayed Antibiotic Prescription for Children With Respiratory Infections: A Randomized Trial. Pediatrics. 2021 Mar;147(3):e20201323. doi: 10.1542/peds.2020-1323. Epub 2021 Feb 11. PMID: 33574163 (Justin’s write up can be found here.)
Bottom line: Delayed antibiotics don’t make sense. Antibiotics don’t magically start treating viruses just because you wait 2 days.
More Peds ID: Tympanostomy tubes don’t work
Hoberman A, Preciado D, Paradise JL, et al. Tympanostomy Tubes or Medical Management for Recurrent Acute Otitis Media. N Engl J Med. 2021 May 13;384(19):1789-1799. doi: 10.1056/NEJMoa2027278. PMID: 33979487
Bottom line: Ultimately, I don’t think this trial definitively proves that there is no role for tympanostomy tubes, but considering that there was never great evidence for the practice in the first place, it really should curtail the practice. At this point, I would want to see a positive study before I subjected my child to surgery.
Back to BaSICS: Normal saline is just fine
Zampieri FG, Machado FR, et al. Effect of Intravenous Fluid Treatment With a Balanced Solution vs 0.9% Saline Solution on Mortality in Critically Ill Patients: The BaSICS Randomized Clinical Trial. JAMA. 2021 Aug 10. doi: 10.1001/jama.2021.11684. PMID: 34375394 [free full text]
People got really excited about the SMART and SALT-ED trials, but they were trials with very imperfect methodology and mixed results. Before BaSICS, the highest quality trial we had was SPLIT, and it also showed no harm from normal saline.
Bottom line: This is the best evidence to date, and there does not appear to be anything harmful about using normal saline as your IV fluid of choice.
Intense oxygen therapy in palliative care: on oxymoron?
Ruangsomboon O, Dorongthom T, Chakorn T et al. High-Flow Nasal Cannula Versus Conventional Oxygen Therapy in Relieving Dyspnea in Emergency Palliative Patients With Do-Not-Intubate Status: A Randomized Crossover Study. Ann Emerg Med. 2020 May;75(5):615-626. doi: 10.1016/j.annemergmed.2019.09.009. PMID: 31864728
Bottom line: There are obviously some limitations, which are discussed in the full blog post, but if you are not already using HFNC for palliation, I think this is good enough evidence to start.
The Evidence-Based Metaphor
Trogen B. The Evidence-Based Metaphor. JAMA. 2017 Apr 11;317(14):1411-1412. doi: 10.1001/jama.2016.17219. PMID: 28399255
“We implement evidence based medicine, so why not evidence based communication?”
The Mindset of the Resuscitationist
Gray SH, Lauria MJ, Hicks C. The Mindset of the Resuscitationist. Emerg Med Clin North Am. 2020 Nov;38(4):739-753. doi: 10.1016/j.emc.2020.06.002. Epub 2020 Jul 23. PMID: 32981614
Danish cowboys: Performing LPs with high INRs
Bodilsen J, Mariager T, Vestergaard HH, et al. Association of Lumbar Puncture With Spinal Hematoma in Patients With and Without Coagulopathy. JAMA. 2020 Oct 13;324(14):1419-1428. doi: 10.1001/jama.2020.14895. PMID: 33048155
Bottom line: In this database, there was no association between coagulopathy and spinal hematoma after lumbar puncture. The rate of spinal hematoma remains about 2/1000 no matter what the labs showed…
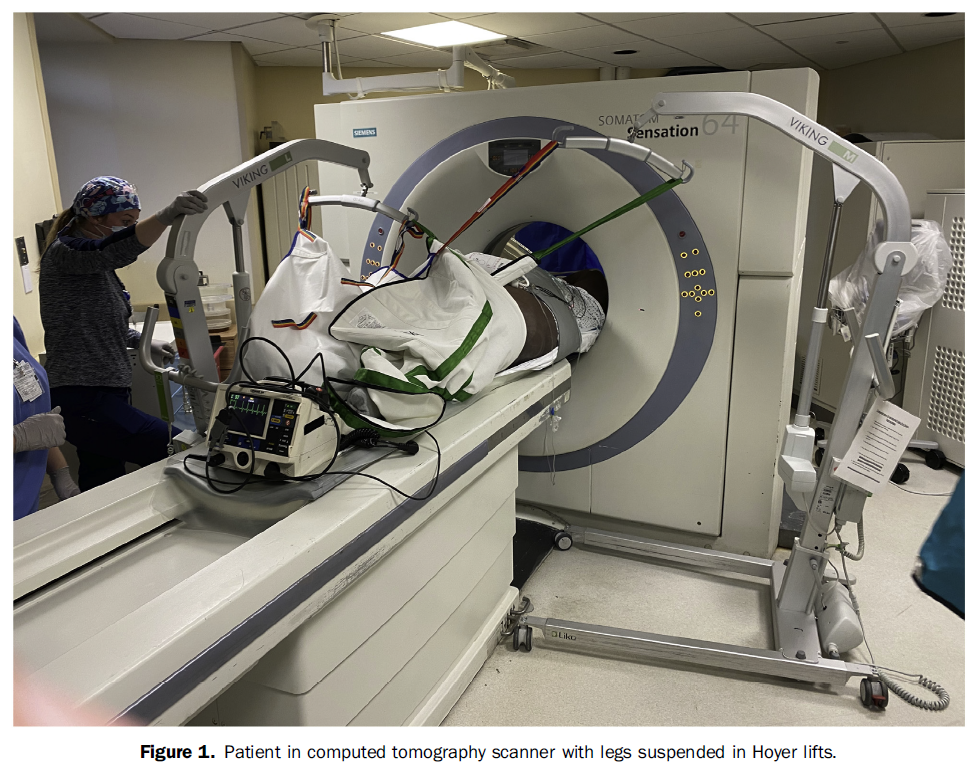
Too big for CT?
Sacchetti AD, Crookshank A, Leidy K. A Novel Solution to Patients Exceeding Weight Limit on Computed Tomography Scanner. Ann Emerg Med. 2021 Aug;78(2):313-314. doi: 10.1016/j.annemergmed.2021.04.012. PMID: 34325866
Bottom line: Hospitals really need to consider the heaviest patients that could present, and not the average patient, when purchasing equipment (and manufacturers need to consider the same when building equipment).
Risk versus harm
Morgan DJ, Scherer LD, Korenstein D. Improving Physician Communication About Treatment Decisions: Reconsideration of “Risks vs Benefits”. JAMA. 2020 Sep 8;324(10):937-938. doi: 10.1001/jama.2020.0354. PMID: 32150219
It’s all about perception
Abidova A, Alcântara da Silva P, Moreira S. Accuracy of Patients’ Waiting Time Perceptions in the Emergency Department. Acad Emerg Med. 2020 Dec;27(12):1348-1349. doi: 10.1111/acem.13949. Epub 2020 Mar 18. PMID: 32103560
About 3 quarters of patients overestimated how long they waited in ED… It has never been a huge priority, but I think we need to rethink HOW patients wait, not just how long they wait.
Hypothermia not looking so hot anymore
Dankiewicz J, Cronberg T, Lilja G, et al: TTM2 Trial Investigators. Hypothermia versus Normothermia after Out-of-Hospital Cardiac Arrest. N Engl J Med. 2021 Jun 17;384(24):2283-2294. doi: 10.1056/NEJMoa2100591. PMID: 34133859
Bottom line: After the pair of TTM trials, we know for sure that hypothermia is not beneficial. Whether fever control, or any temperature management, is effective remains an open question, but that is a hypothesis untested by RCTs. Based on data in other critically ill patients, it is very unlikely that fever control improves outcomes, but I imagine we will see RCTs on that in the future. Justin’s full write up can be found here.
See you soon for more EBM and nerdiness
Casey
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS

Hypercalcemia in a nutshell
Clinical Case 012: Obstetric challenge

Broome Docs Podcast: the “difficult historian” rant
About The Author
Casey Parker
I am a GP working in Broome, NW of Western Australia. I work as a hospital DMO (District Med Officer) doing Emergency, Anaesthestics, some Obstetrics and a lot of miscellaneous primary care. Also on the web as @broomedocs | + Casey Parker | Contact