First10EM Journal Club: August 2020
Welcome back for another month of nerdy Nirvana with Dr Justin Morgenstern. This month on the journal club we cover TXA for GI, Dex for COVID, pinky ladies (again) and haloperidol for headaches… plus a bunch of other goodies that just might make your job easier.
As always there are free PDF copies of the papers we discuss linked below. As my friend Ken says – be skeptical, even if you hear it here… actually especially of you hear it here.
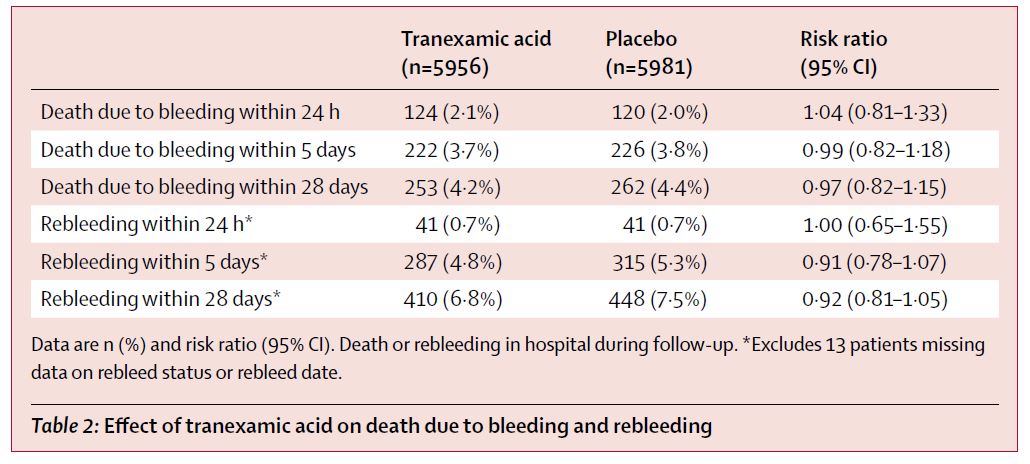
HALT-IT Trial Collaborators. Effects of a high-dose 24-h infusion of tranexamic acid on death and thromboembolic events in patients with acute gastrointestinal bleeding (HALT-IT): an international randomised, double-blind, placebo-controlled trial. Lancet. 2020;395(10241):1927-1936. doi:10.1016/S0140-6736(20)30848-5 PMID: 32563378
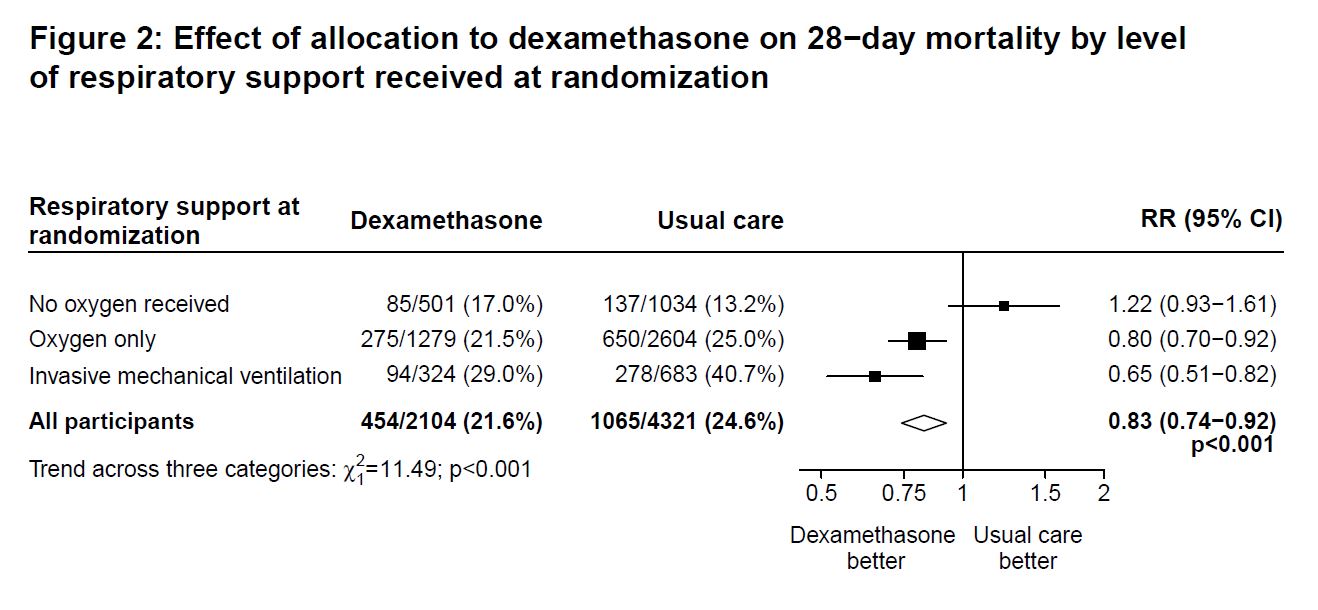
RECOVERY Collaborative Group, Horby P, Lim WS, et al. Dexamethasone in Hospitalized Patients with Covid-19 – Preliminary Report. N Engl J Med. 2020;10.1056/NEJMoa2021436. doi:10.1056/NEJMoa2021436 PMID: 32678530
You can read more here. and HERE too
Carley S, Horner D, Body R, Mackway-Jones K. Evidence-based medicine and COVID-19: what to believe and when to change. Emerg Med J. 2020;emermed-2020-210098. doi:10.1136/emermed-2020-210098 PMID: 32651176
Warren J, Cooper B, Jermakoff A, Knott JC. Antacid monotherapy is more effective in relieving epigastric pain than in combination with lidocaine. A randomized double-blind clinical trial. Acad Emerg Med. 2020;10.1111/acem.14069. doi:10.1111/acem.14069 PMID: 32602148
There are prior RCTs saying the same thing.
Lindblad AJ, McCormack J, Korownyk CS, et al. PEER simplified decision aid: osteoarthritis treatment options in primary care. Can Fam Physician. 2020 Mar; 66(3):191-193. Available at: https://www.cfp.ca/content/66/3/191
McCoy JJ, Aldy K, Arnall E, Petersen J. Treatment of Headache in the Emergency Department: Haloperidol in the Acute Setting (THE-HA Study): A Randomized Clinical Trial. J Emerg Med. 2020;S0736-4679(20)30349-8. doi:10.1016/j.jemermed.2020.04.018 PMID: 32402480 NCT02747511
Zulman DM, Haverfield MC, Shaw JG, et al. Practices to Foster Physician Presence and Connection With Patients in the Clinical Encounter [published correction appears in JAMA. 2020 Mar 17;323(11):1098]. JAMA. 2020;323(1):70–81. doi:10.1001/jama.2019.19003 PMID: 31910284 [article]

My talk from SMACC GOLD entitled: The History of Empathy is worth a listen if you are interested in the science behind empathy and patient connection. There is some good data that we can improve our care with simple empathy.
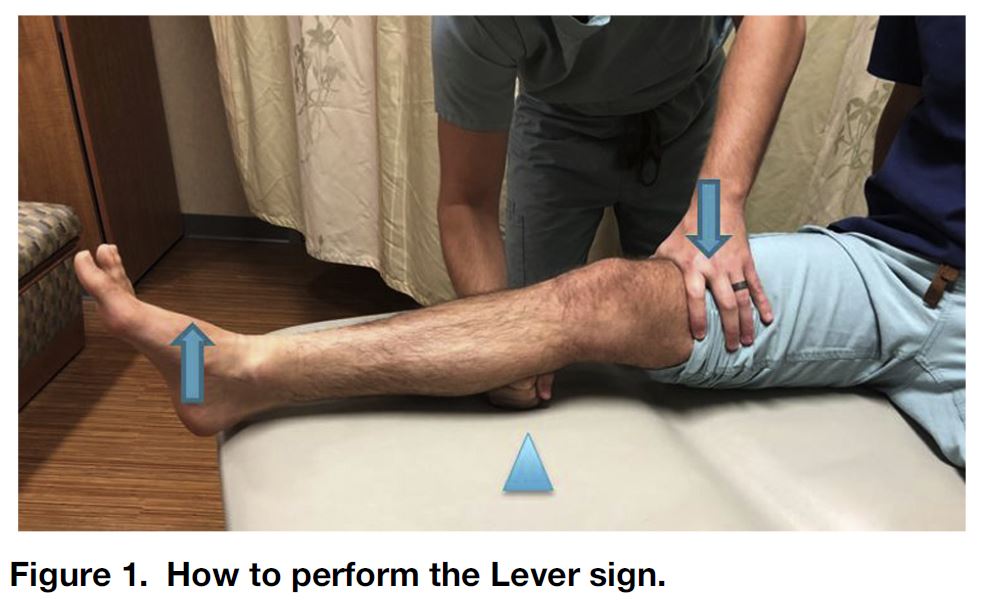
McQuivey KS, Christopher ZK, Chung AS, Makovicka J, Guettler J, Levasseur K. Implementing the Lever Sign in the Emergency Department: Does it Assist in Acute Anterior Cruciate Ligament Rupture Diagnosis? A Pilot Study. J Emerg Med. 2019;57(6):805-811. doi:10.1016/j.jemermed.2019.09.003 PMID: 31708315
Tran QK, Rehan MA, Haase DJ, Matta A, Pourmand A. Prophylactic antibiotics for anterior nasal packing in emergency department: A systematic review and meta-analysis of clinically-significant infections. Am J Emerg Med. 2020;38(5):983-989. doi:10.1016/j.ajem.2019.11.037 PMID: 31839514
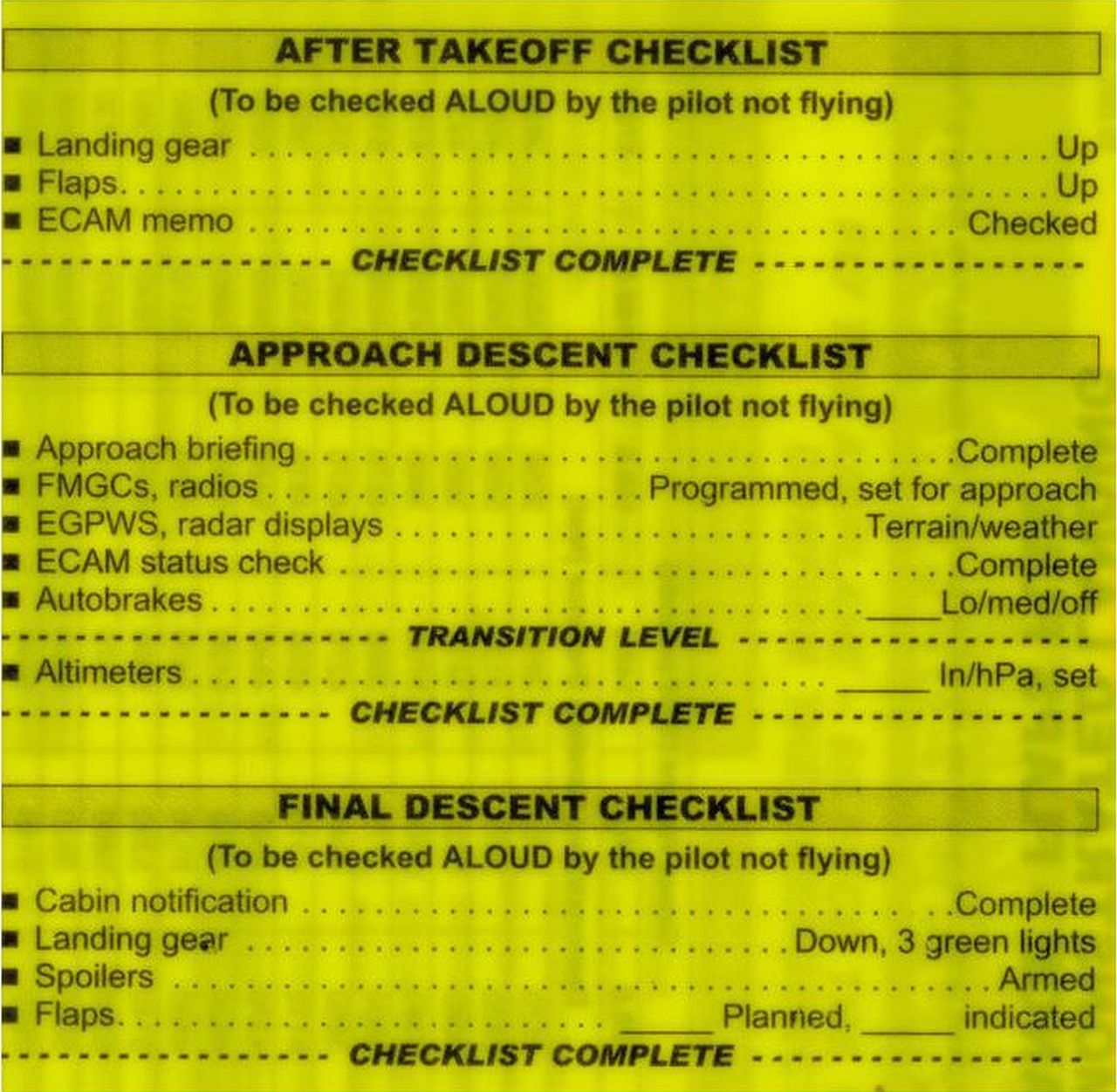
Turner JS, Bucca AW, Propst SL, et al. Association of Checklist Use in Endotracheal Intubation With Clinically Important Outcomes: A Systematic Review and Meta-analysis. JAMA Netw Open. 2020;3(7):e209278. Published 2020 Jul 1. doi:10.1001/jamanetworkopen.2020.9278 PMID: 32614424
For a great talk on airway checklists, check out My Checklists Manifesto by Michael Lauria: https://www.youtube.com/watch?v=36vgGdxKkPQ&feature=youtu.be
The SMACC Airway Checklist debate is still going… but you can catch the first 20 minutes here:
Catchpole K, Russ S. The problem with checklists. BMJ Quality & Safety 2015;24:545-549. DOI: 10.1136/bmjqs-2015-004431
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS
Clinical Case 097: Paediatric Short case

SMACC is here

Clinical Case 121: Supracondylar Sono Subtlety
About The Author
Casey Parker
I am a GP working in Broome, NW of Western Australia. I work as a hospital DMO (District Med Officer) doing Emergency, Anaesthestics, some Obstetrics and a lot of miscellaneous primary care. Also on the web as @broomedocs | + Casey Parker | Contact
CommentGreat podcast guys and in particular excellent discussion of the RECOVERY trial including using EBM 2.0 methodology!
Given your pre-TP estimates you found using Bayesian analysis the likelihood of the clinical hypothesis (that Dex saves lives in COVID) being true is 70-90% depending on whether you were conservative or optimistic with your pre-test probability (prior probability). However as you point out that’s before considering both visible bias (VB) and invisible bias (IB). Re visible bias Justin points out the lack of blinding as big issue. The other issue which was to some extent unavoidable was the lack of a pre-specified sample size which can give researches flexibility to stop the trial at the point during random data fluctuation where the benefit (and attendant p value) looks best. ANY flexibility in a trial design increases the risk that your finding is a false positive.
Regarding invisible bias, the evidence shows there is always a significant risk of invisible bias in the design, conduct, analysis and presentation of results, especially in an unblinded study. However invisible publication bias is also potentially significant here. Given how early we knew that the massive inflammatory response was the cause of death, Dex was one of the most obvious candidates for an RCT – as such it is utterly inconceivable that there have not been other (albeit probably smaller) RCTs on Dex in COVID which makes you wonder why have we not seen them? Almost always the reasons for trials not being published is that they are “negative”. Particularly in a COVID world where doctors are overwhelmed with patients, it may not be that motivating if you studied Dex and the result was negative to spend your few hours where you need to sleep writing up a paper and that’s aside from whether you believed it might actually be published in a competitive market.
Overall then, if you discounted for both VB and IB your post test probabilities are likely to be somewhat lower than the 70-90% range suggested.
Is it reasonable to change practice now despite this? I think so. It is a cheap and well known drug with a well established side effect profile. However doing so should NOT preclude studying this against placebo to REPRODUCE the findings as the “one and done” culture in EBM is harmful to the pursuit of science and ultimately our patients. That’s a key aspect of adhering to the ASA’s concept of “Accepting Uncertainty” – deciding what to do now while the truth remains uncertain but while we continue to pursue the truth.
Thanks again for a great podcast.
More on the EBM 2.0 approach at EBM2point0.com
Our review of pink lady to treat epigastric pain
http://thesgem.com/2020/09/sgem302-we-didnt-start-the-fire-but-can-antacid-monotherapy-stop-the-fire/