First10EM Journal Club: January 2020
It is a New Year and Justin is back on the podcast to discuss another series of papers that range from serious science to silly stuff.
We had a great time recording this podcast, so many things learned. Hope you enjoy it too.
The papers as ever are below in free PDF format and the audio is at the bottom. This episode does involve a lot of visual descriptions of ECGs, ECHOs and jujitsu manoeuvres – so you might want to check out the papers to understand what the heck we are talking about!
OK, here we go:
ESETT: Kapur J, Elm J, Chamberlain JM, et al. Randomized Trial of Three Anticonvulsant Medications for Status Epilepticus. The New England journal of medicine. 2019; 381(22):2103-2113. PMID: 31774955
Bottom line: There was no difference between levetiracetam, valproate, and fosphenytoin as the second line agent in status epilepticus.
Peck D, Al-Kaisey A. Cardiac memory: an under-recognised cause of deep T wave inversion in a patient presenting with chest pain. BMJ case reports. 2018; :. PMID: 30061136
Gautschi O, Naegeli B. Cardiac memory mimicking myocardial ischaemia. Journal of the Royal Society of Medicine. 2003; 96(3):131-2. PMID: 12612116
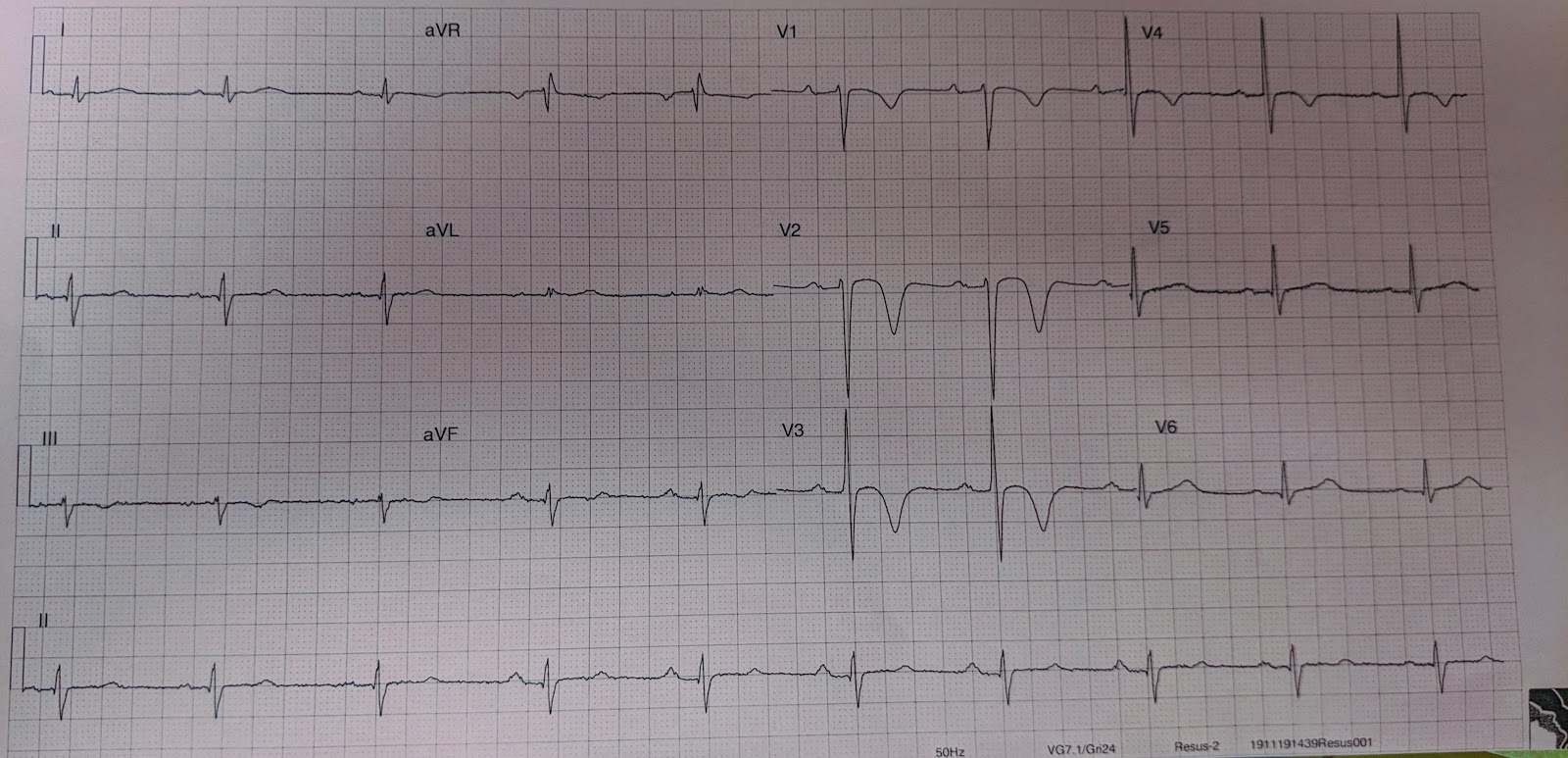
The ECGs that Justin describes in his case are here: Firstly, deep septal TWI….
ECG #1
When we repeated the ECG, it had changed. Now there was a left bundle branch block, with conchordant ST changes…
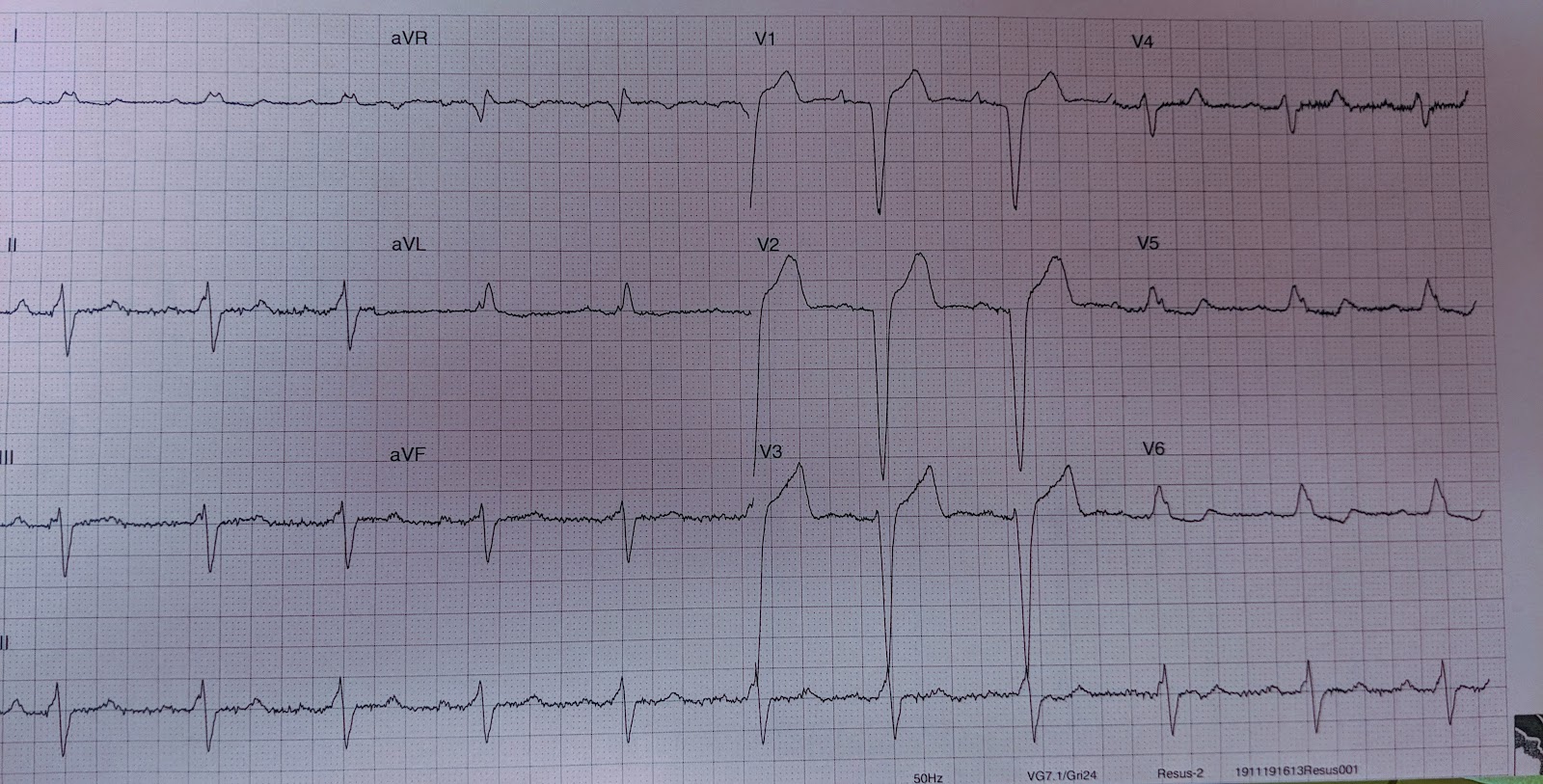
I was baffled, so I turned to Twitter for some help. It was Sam Ghali (@EM_RESUS) that ultimately came up with what I believe to be the right diagnosis: cardiac memory. I had never heard of “cardiac memory” before. (It is also sometimes called “Chatterjee phenomenon”.) Apparently after being in a ventricular rhythm, the T wave “remembers” or tends to persist along the same vector. The result is that you can get deep T wave inversions just like I saw. Apparently this is very common after pace-makers, but it can also happen after an intermittent left bundle branch block, like we saw in my case. It is generally considered benign.
Wren C, Campbell RW, Hunter S. Role of echocardiography in differential diagnosis of broad complex tachycardia. British heart journal. 1985; 54(2):166-72. [pubmed]
Pancaro C, Shah N, Pasma W, et al. Risk of Major Complications After Perioperative Norepinephrine Infusion Through Peripheral Intravenous Lines in a Multicenter Study. Anesthesia and analgesia. 2019; PMID: 31569163
Bottom line: I think we are likely to see much higher rates of extravasation in the ED, but because true harms are rare, the overall message is still correct: if monitored carefully, it is perfectly reasonable to give norepinephrine through a well functioning peripheral IV.
Crawford SN, Lee LS, Izuka BH. Closed treatment of overriding distal radial fractures without reduction in children. The Journal of bone and joint surgery. American volume. 2012; 94(3):246-52. PMID: 22298057
Bottom line: Pediatric fractures undergo a tremendous amount of remoulding. We might be overdoing our reductions somewhat, especially now that sedations are relatively easy to perform in most EDs.
Tsze DS, Woodward HA. The “Facemask Blinder”: A Technique for Optimizing Anxiolysis in Children Undergoing Facial Laceration Repair. Pediatric emergency care. 2019; 35(7):e124-e126. PMID: 27941503
For more tips and tricks on making hospitals less scary, see this post.
Meek R, Mee MJ, Egerton-Warburton D, et al. Randomized Placebo-controlled Trial of Droperidol and Ondansetron for Adult Emergency Department Patients With Nausea. Academic emergency medicine. 2019; 26(8):867-877. PMID: 30368981
Bottom line: Our anti-emetics probably aren’t as effective as we like to think, but they are probably better than this trial makes them seem.
Slevin JP, Harrison C, Da Silva E, White NJ. Martial arts technique for control of severe external bleeding. Emergency medicine journal : EMJ. 2019; 36(3):154-158. PMID: 30612092
Gunnerson KJ, Bassin BS, Havey RA, et al. Association of an Emergency Department-Based Intensive Care Unit With Survival and Inpatient Intensive Care Unit Admissions. JAMA network open. 2019; 2(7):e197584. PMID: 31339545 [free full text]
Bottom line: Don’t redesign your hospital yet, but conversations between ICU and ED to ensure processes are in place so that patients get the best possible care no matter where they are physically situated sound like a good idea.
Brookfield CR, Phillips PPJ, Shorten RJ. Q fever-the superstition of avoiding the word “quiet” as a coping mechanism: randomised controlled non-inferiority trial. BMJ (Clinical research ed.). 2019; 367:l6446. PMID: 31852676 [free full text]
Podcast: Play in new window | Download
Subscribe: Apple Podcasts | RSS

November 2016: First10EM / Broomedocs Journal Club

Appendicitis: Surgery vs. Antibiotics

Clinical Case 068: Surviving sepsis. Serial scans for super-sick sheila
About The Author
Casey Parker
I am a GP working in Broome, NW of Western Australia. I work as a hospital DMO (District Med Officer) doing Emergency, Anaesthestics, some Obstetrics and a lot of miscellaneous primary care. Also on the web as @broomedocs | + Casey Parker | Contact